Improvement of Circulation Using The Radial Appliance Douglas G. Richards, Ph.D., David McMillin, M.A., Carl Nelson, D.C., & Eric Mein, M.D. Meridian Institute
[NOTE: This article was published in Subtle Energies and Energy Medicine,
Vol. 7, No. 1, 1996; see
below for continuing
education credit for this article.]
Abstract The purpose of this study was to determine if a subtle energy device, the Cayce Radial Appliance, could improve circulation in the extremities. There were two aspects to the study: a double-blind, placebo-controlled experiment and a small clinical investigation. In the experiment, 30 subjects were selected for cold extremities, with the criterion that either the hands or the feet had to be below 80 degrees F during the initial measurement session. To measure improvement of circulation, we used digital thermometers to record the temperatures of the thumbs and big toes on both hands and feet. Subjects were instructed to use the appliance 16 times; laboratory measurements were taken during the 1st, 4th and 16th sessions. Skin temperature turned out to be a difficult variable to work with, due to the wide variability in temperature apparently not related to the experimental situation. The strongest results were observed in the 4th session. During the session baseline, the difference between hand and foot temperatures of the experimental group was significantly higher than that of the control group (t(13,11) = 2.49, p = .02). The 16th session did not yield significant differences between the experimental and control groups. However, in the experimental group, there was a correlation of r(9) = -.56 (p = .07) of hand temperature increase with the number of days it took to complete the 16 sessions. That is, those subjects who were more consistent in using the appliance may have obtained better results, though statistically the result is only suggestive due to the small sample size. In contrast, in a clinical follow-up study with five subjects and no control group, we found that all subjects had a substantial increase in hand temperature following three sessions on the appliance (Mean increase = 8.4 degrees F, SD = 3.3). This increase was well in excess of that seen in either the experimental or control groups in the previous study. One important difference was that in the clinical study, use of the appliance was closely supervised, whereas in the blind study most of the appliance sessions were conducted by the subjects alone in their homes. Keywords: circulation, temperature, Cayce, Radial
Appliance
Introduction The Radial Appliance is an electrical device intended to balance the subtle energies of the body. It was developed by a group of inventors in the 1920s and 1930s with guidance from the Edgar Cayce readings. Edgar Cayce has been acknowledged in an editorial in the Journal of the American Medical Association as the originator of holistic medicine.1 Yet despite widespread application of Cayce's principles, few have been tested in controlled situations. While in a trance state, Edgar Cayce gave over
14,000 discourses on health and other topics, known as readings.
The first Cayce reading on the Radial Appliance was given on July 27, 1925
for Thomas Brown, a businessman from Akron, Ohio (Reading 1800-4).2
Over the next 15 months, Brown obtained 10 more readings on all aspects
of construction and therapeutic application. Cayce encouraged him
to experiment and come up with improvements, and would then critique those
improvements. Several more experimenters worked with the device.
The design in this study is based on the accumulated knowledge ending with
the last appliance reading on October 14, 1941 (Reading1800-33).2
In Cayce's time the most common name for the device was the "Radio-Active"
Appliance; in the pre-atomic energy era, radioactivity was considered to
be a benign force, although the appliance contained no radioactive elements.
We have chosen to call it the "Radial" Appliance in this study, based on
the "radial action" to the extremities. McMillin and Richards3
give more details on the history of the appliance. In the form used
in this study, the Radial Appliance consists of two pieces of "60%" carbon
steel (0.6% or 1060 steel), separated by two pieces of glass, surrounded
by carbon blocks and charcoal, and sealed in a brass container. Electrically
the device is a capacitor, and produces no voltage of its own. It
is "activated" by being placed in ice water. The steel plates are
connected to the body by wires with electrodes made of German Silver (a
nickel alloy). Figure 1 is a diagram of the
construction of the appliance.
The appliance is similar in construction and use to the Eeman biocircuit, a device invented in the 1920s by L. E. Eeman.4 Substantial anecdotal evidence exists for the efficacy of the Eeman device.5 In addition, a double-blind, placebo-controlled study by Isaacs and Patten has shown the Eeman device to significantly change both subjective states and physiological measurements.6 Like the Eeman device, the Cayce appliance produces no voltage and relies on the body's own electricity for its effect. A small study at the Fetzer Energy Medicine Research Institute yielded promising preliminary results with the Cayce Radial Appliance affecting blood chemistry.7 The Cayce appliance was recommended frequently in the readings (933 times), often for relaxation and "equalization of circulation." Specifically, in a number of readings, the appliance was supposed to improve poor circulation for people with cold hands and feet: "We would also use, in the REST periods - which should be taken each day - the Radio-Active Appliance, that makes for COORDINATIONS from the distresses in the extremities. This will relieve that tendency of cold feet, that tendency of the poor circulation in the extremities." (Reading 326-1)2 Unlike many Cayce prescriptions, which were specific for individuals, the Radial Appliance had widespread application: "The Radio-Active battery would be good for EVERYBODY!...This assists in keeping an equilibrium." (Reading 202-7)2 Cayce also recommended the appliance as part of the treatment for many specific disorders, among them migraine headaches. By re-directing blood flow to the hands, in a manner analogous to the now commonly used temperature biofeedback, the appliance could help in reducing headaches. Anecdotal reports over the years have suggested that the appliance is useful for improving circulation. However, since the use of the appliance includes hour-long relaxation periods while the person is connected to the device, we felt it important to assess the contribution of the placebo effect as well as clinical outcomes. Experimental Study The purpose of the experimental study was to determine if the effects of the appliance on circulation could be measured using the temperature of the extremities, under double-blind conditions. Our criterion for the subjects in this study required only cold hands or cold feet. Since Cayce said the appliance would be good for everybody, the presence or absence of a specific disease was not a criterion for inclusion or exclusion. We hypothesized that there would be differences between the experimental and control groups including (1) overall increases in the temperature of the extremities, and (2) changes in the temperature difference between the hands and the feet. Method Subjects The subjects were volunteers who identified themselves as having cold hands or feet. The nature, potential benefits, and potential risks of participating in the study were explained to prospective subjects, and were detailed on a written consent form. For some subjects, there was a screening process in which they measured the temperatures of their own extremities at home. For the others, the screening was performed during the first measurement of baseline temperature in the laboratory. The screening criterion was that either the hands or feet had to be below 80 degrees F, measured at the thumb and big toe. There were 4 male subjects and 26 female subjects; the mean age was 48.9 (SD = 14.1). One male subject was dropped from the study during the initial baseline when his temperatures rose above the criterion; we continued to collect data, but did not include it in the analysis. Several other subjects were excluded from the data analysis at later times, as explained in the results section. The temperature differences between experimental and control groups in the initial baseline were not statistically significant (See Results and Table 2). There was no restriction as to the medical condition causing the cold hands or feet. Most of the subjects had never been diagnosed with any medical condition affecting circulation. Some had been diagnosed with circulatory problems such as diabetes or Raynaud's syndrome. Others had medical conditions that could conceivably affect circulation such as high blood pressure, lupus erythematosus, and Parkinson's disease. Appliances Radial Appliances were obtained from Tom Dewey (Dewey Transformational Technologies, 1168 First Colonial Road, Suite 7, Virginia Beach, VA 23454). They were constructed according to the specifications in the Cayce readings (1800 series) as discussed in McMillin and Richards.3 All appliances were identical. Half were turned into placebo devices by construction of plugs with unconnected wires inside, filled with epoxy. The wires were divided randomly into two groups by an independent research assistant who kept the key during the duration of the experiment. The researchers having contact with the subjects were not aware of which subjects had the experimental or control wires. The appliances and their wires were numbered consecutively from 1 to 30, and were assigned to subjects in the order of their entry into the project. Session Protocol The temperatures of each subject were measured in the laboratory three times. Each session lasted 2 hours. All sessions were scheduled in the afternoon and early evening to minimize the effect of diurnal body temperature variations. (Body temperature is relatively steady during these hours, but drops during the night, and rises again in the morning.) The subjects used the appliances at home for 13 times, for 1 hour each time. The sequence of laboratory and home sessions is given in Table 1. Session 1 The subject would arrive at the laboratory. The researcher would follow a checklist to conduct the session, checking off each step as it was performed. These steps included: - explanation of the project and filling out of
forms, including informed consent (15 minutes),
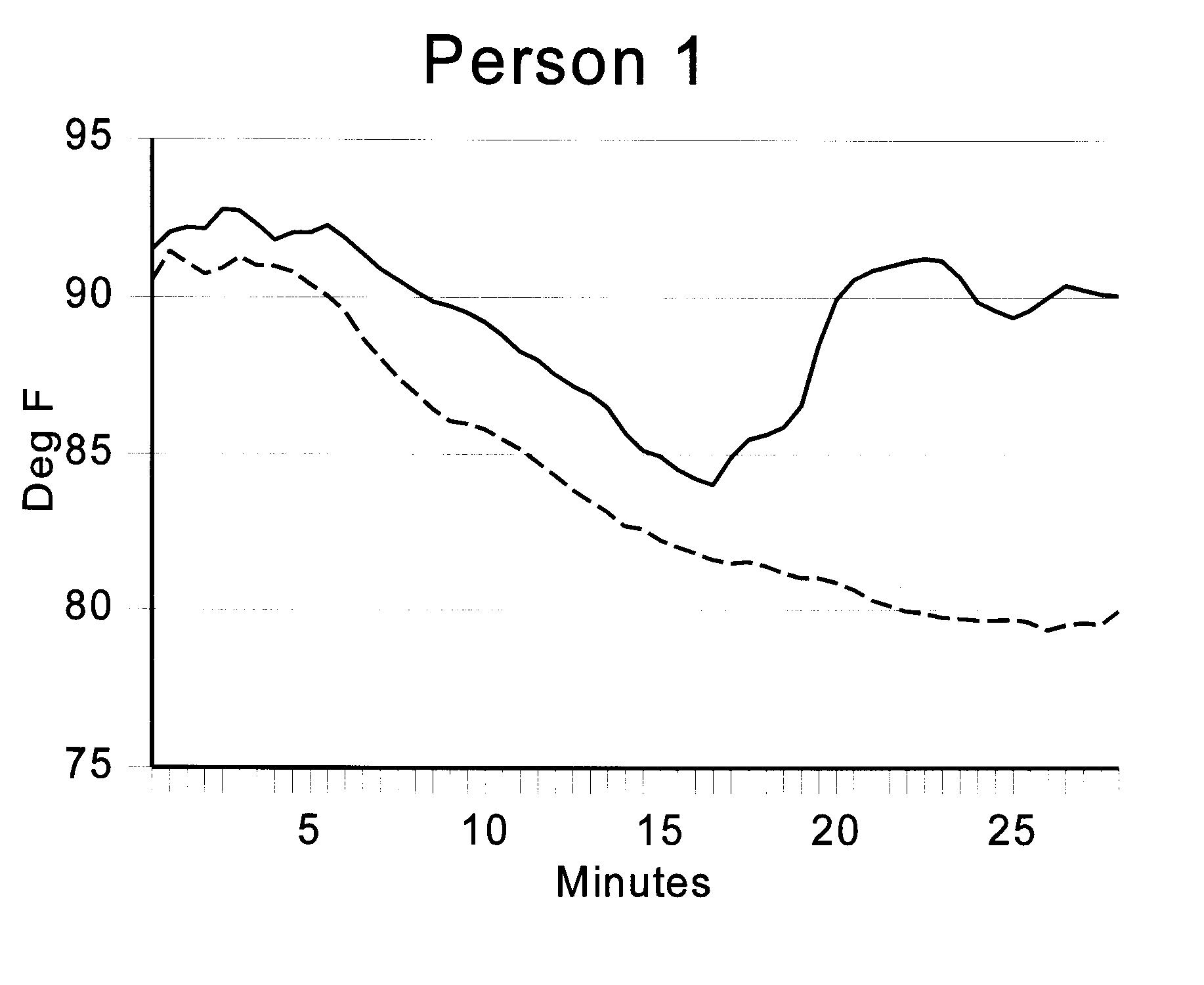
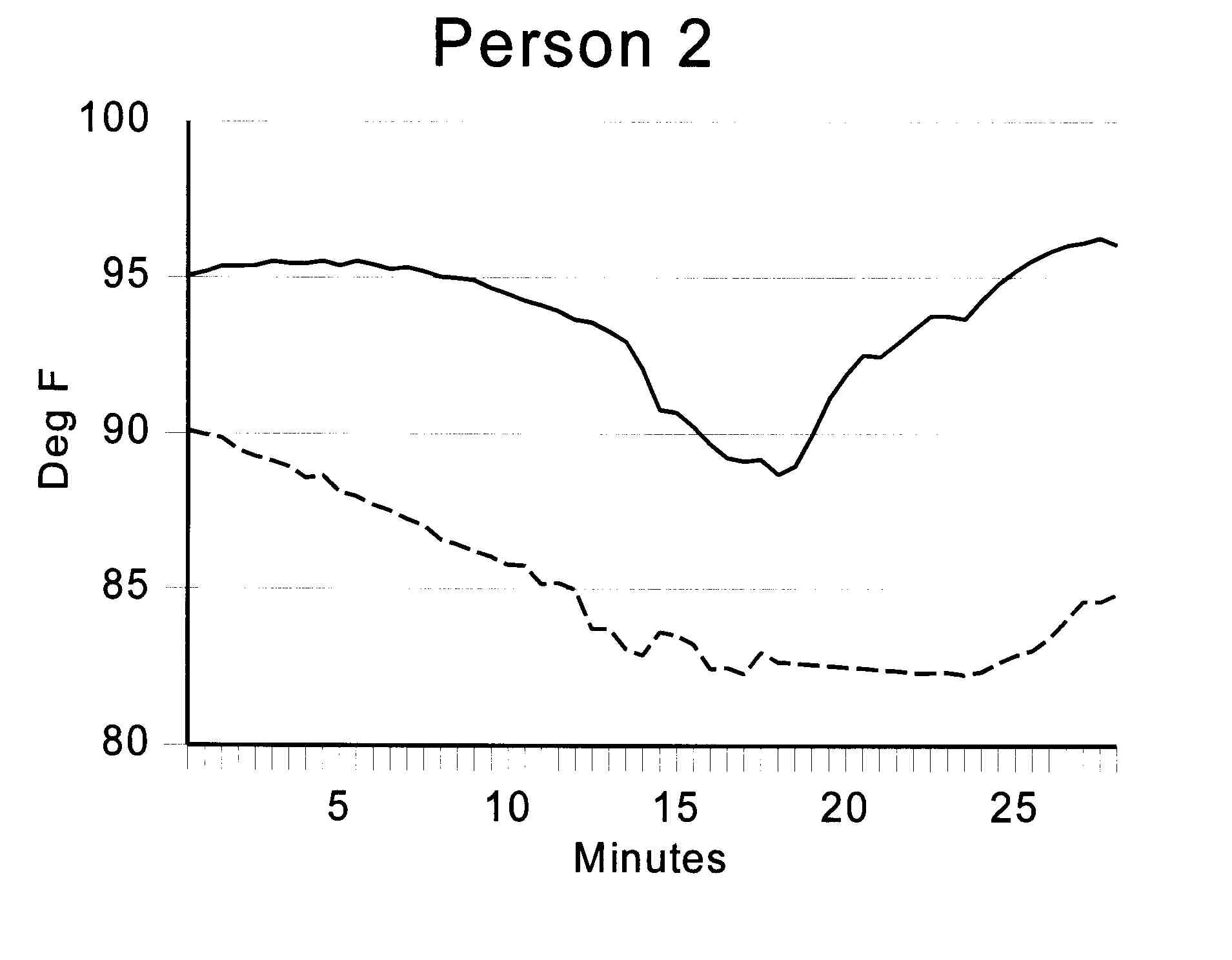
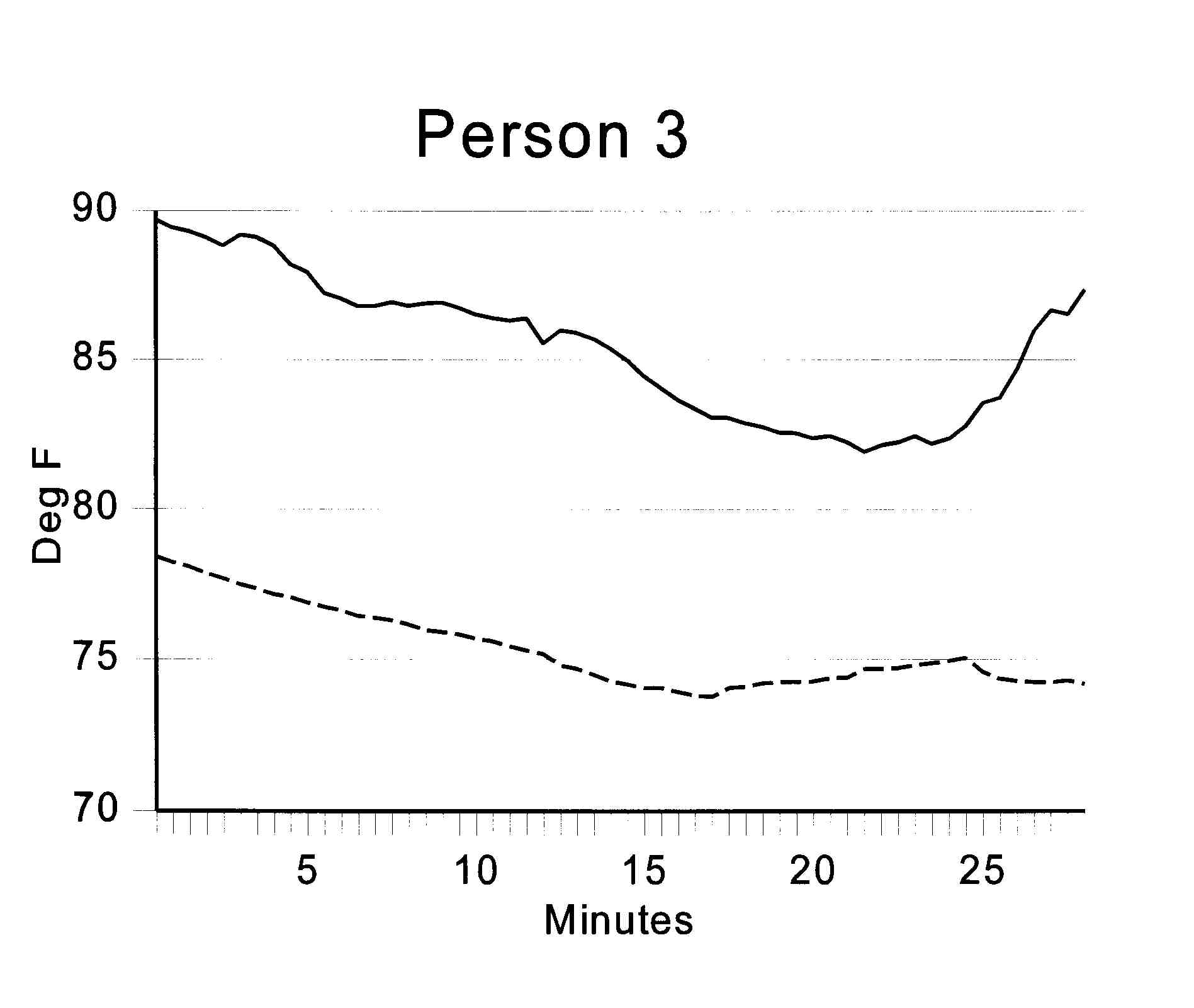
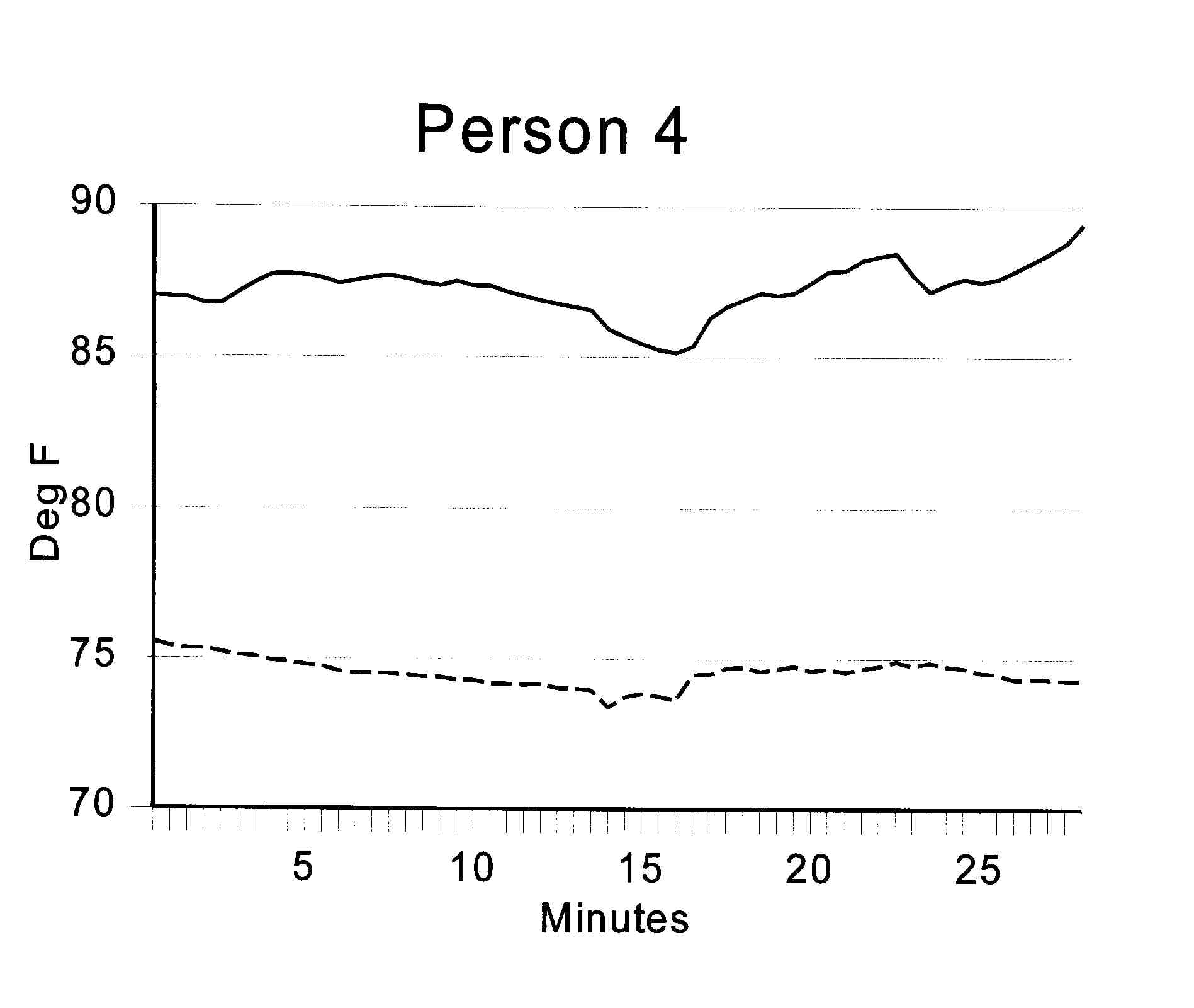
Timing of the sessions was adhered to rigorously in order to minimize variability due to outdoor temperature. The first baseline temperature measurements of the extremities were made exactly 15 minutes after the subject entered the laboratory, and every 10 minutes thereafter. At the beginning of the baseline period and the end of the session, questionnaires were completed by the subjects on their subjective perception of relaxation, as well as hand, foot, and overall temperature. At the end there was a question on subjective opinion of whether the appliance was real or a placebo. Sessions 4 and 16 The same procedure used for Session 1 was followed, but the filling out of forms and explanations of the project were eliminated. Time was allowed for the subject to ask questions and practice setting up the appliance, if necessary. Laboratory Measurement Temperatures were measured using digital thermometers with fast-responding sensors (2 second response time). The thermometers (Model No. SC911 - Conscious Living Foundation, Drain, Oregon) are standard indoor/outdoor thermometers, sold for biofeedback training. The specifications list an accuracy of +- 1.8 degrees F. Since we desired greater accuracy, we obtained 10 thermometers and calibrated them against each other at both ends of the range of interest (68 degrees to 96 degrees). Calibration consisted of taping the sensors to skin (big toe for 68 degrees and underarm for 96 degrees). Six of the 10 thermometers matched within 0.2 degrees, and were used to measure the room temperature, the temperatures of the extremities, and the outdoor temperature. The following measurements were taken every 10 minutes: room temperature, each hand, and each foot. Mouth temperature was taken at the beginning of the baseline period and at the end of the session (there was no consistent variation and it is not included in the Results section). Outdoor temperature in the shade was taken once in the middle of the session using one of the calibrated digital thermometers. Room temperature was maintained at between 68 and 72 degrees F. A heat pump providing both heating and air conditioning was used. The blower was left on continuously to provide a smooth background noise, and to prevent layering of temperature in the room. Measured mean room temperature was not significantly different among the three sessions, and was 70.5 degrees F (SD = 0.4). Home Use of Radial Appliances We based the protocol for home use of the appliances on the advice in the Cayce readings. The readings suggest that the appliance should be used for a minimum of one hour at a session, while resting quietly. It can be used as frequently as every night, and in general was recommended to be used at least 4 times per week. Preliminary measurements with a single subject suggested that substantial temperature changes might be seen by the fourth session. Subjects were given instructions for home use of the appliance and supervised in practice during their first session. They were told to use the appliance twice before their next session in the lab, which would be their fourth session on the appliance. Following that session in the lab, they were instructed to use the appliance 11 more times, and come back for a final session in the lab within a month. An appointment was made during the second session for the final session. Thus, if correctly following the protocol, the subject would use the appliance a total of 16 times within a month. The minimum time in which this could be completed was 16 days, if the appliance was used every day. For each time of use, the subjects were provided with a data sheet giving instructions for the attachments of the electrodes, and questions about their appliance use. Results We used a pretest/posttest design, in which the changes from the Session 1 baseline period (prior to the first connection to an appliance) would be compared between experimental and control groups for Sessions 4 and 16. Since this was an exploratory study, and we were interested in all possible effects, we also looked at absolute differences in temperature in Sessions 4 and 16 between experimental and control groups. Because of variability in subject compliance with the protocol, the changes between Sessions 1 and 4, and Sessions 1 and 16 are analyzed separately, rather than being combined in a method such as repeated measures analysis of variance. Most subjects complied well with the protocol during the first week, but following Session 4 there was wide variation in the time taken to complete all the home sessions. The effect of this variability is analyzed later in the results section. For each laboratory session 40 measurements of extremity temperature were taken (4 limbs x 10 ten-minute time intervals). Selection of an appropriate dependent variable presents some challenges, since the measurements are highly correlated. Prior to breaking the double-blind condition, we made the following decisions for data reduction: Baseline Temperature. To minimize the effects of outdoor temperature, the final two 10-minute measurements in the baseline period were averaged to yield the "baseline" temperature for each extremity. Including the 15-minute interval prior to the baseline, these measurements were taken 35 and 45 minutes after the subject entered the laboratory. Final Temperature. The "final" temperature for each extremity was the average of the last two temperature measurements in the session; that is, after being attached 50 and 60 minutes to the appliance. In general, there was very little change between 50 and 60 minutes. This average was intended to smooth out any brief temperature variations. Left/Right Averaging. The left/right temperature differences in the subjects were generally small, so for the analysis, the hand and foot temperatures given are averages of the left and right extremities. To simplify the data presentation, in all but one case the baseline temperatures are used for each session, rather than the final temperatures, because the differences between sessions and groups are more pronounced in the baseline condition. The trend of the final temperatures is the same as that of the baseline temperatures, but the magnitude is less. This is due to a general cooling and convergence of the temperatures of the extremities during prolonged measurement in a cool room, an effect reported by Yates.8 Of the 30 subjects enrolled in the study, 29 completed Session 1, 26 completed Sessions 1 and 4, and 23 completed all three laboratory sessions and the 11 home sessions according to the protocol. Session 1 (1st Laboratory Session) Baseline Temperatures During the baseline period, none of the variables differed significantly between the experimental and control groups (Table 2). Session 4 (2nd Laboratory Session) Baseline Temperatures Changes From Session 1 to Session 4. In both the experimental and control groups, the hands and feet increased in temperature from Session 1. For the hands, the increase in the experimental group was over three times greater than in the control group, but the difference between groups was not significant for the hands or the feet, due to the wide range of variability in both groups. The difference between the hands and the feet was also not significant. See Table 3. Absolute Temperatures In Session 4. When absolute temperatures are used, rather than the change in temperature, there is a significant difference between the experimental and control groups in the hand-foot temperature difference. This is primarily due to hand warming, as evidenced by the almost significant difference in absolute hand temperatures between the experimental and control groups. There was no difference in the foot temperatures. See Table 4. Relationship To Outdoor and Room Temperatures. The correlations of all of the dependent variables with outdoor and room temperature were low and not significant. (Mean correlation with outdoor temperature, r = .03; mean correlation with room temperature, r = -.07.) This demonstrates that the room temperature was held sufficiently steady as to not be an influence in the results, and that the combination of the pre-baseline and baseline periods was sufficient for elimination of the effects of outdoor temperature. Session 16 (3rd Laboratory Session) Temperature Changes By Session 16, the differences between experimental and control groups were no longer significant, either in comparison with temperatures in Session 1, or in absolute terms (Tables 5 and 6). Relationship To Outdoor and Room Temperatures. In contrast with Session 4, the difference in outdoor temperatures (but not room temperature) between Sessions 1 and 16 did have a significant correlation with the baseline hand temperature difference (r(21) = .58, p = .004). There was no significant difference between the experimental and control groups, however (t(11,10) = 1.26, p =.22). These correlations with outdoor temperature were gone by the final temperature measurement at the end of the session. Despite explicit instructions on consistent use of the appliance, between Sessions 4 and 16 many subjects found it difficult to use the appliance as frequently as recommended. Some took as long as 46 days to complete the experiment (vs. the intended 30 maximum), and reported that they had had gaps in their appliance use of up to 2 weeks. Rather than exclude them from the study, which would have left too few subjects for any meaningful analysis, we decided to look at the possible contribution of frequency of use to the results. Temperature differences between Sessions 1 and 16 were correlated with the number of days to complete the experiment. For the experimental group, final hand temperature difference, there was a suggestive correlation of r (9) = -.56, p = 07. For the control group, r (10) = .07, p = .83. Thus, in the experimental group, but not in the control group, consistent use of the appliance may well have had an effect on the final temperatures. While only statistically suggestive, this is an important result for design of future protocols. Since there were also some previous correlations with outdoor temperature, a partial correlation of temperature difference vs. number of days to complete the experiment was calculated, corrected for outdoor temperature. For the experimental group, r(9) = -0.52 (p = .12), only slightly less than the uncorrected correlation, suggesting that the outdoor temperature made little difference in the result. Subjective Measure Subjects were asked after each laboratory session to rank, on a 1-7 scale, whether they felt their appliance was real or a placebo. There were no significant differences between the experimental and control groups on this measure, for any of the three laboratory sessions. It is not surprising that the subjects were unable to detect a subjective effect, since the Cayce readings state: "There will be little or no feeling except as the body uses this period for meditation." (Reading 5047-1)2 Clinical Study The purpose of the clinical study was to assess the effectiveness of a holistic set of Cayce therapies for migraine headaches, of which the Radial Appliance was a part. Here we report only on the effects on hand temperature. Method Subjects Five subjects (all female, mean age = 53.9, SD = 9.3), all previously diagnosed with migraine headaches, enrolled in a 10-day residential treatment program employing Cayce therapies. Procedures On the initial day of the program, all subjects received physical examinations, including measures of a variety of autonomic nervous system parameters during a 28-minute session. Only the results of finger temperature are reported here. Continuous temperature measurements were made using a thermistor sensor connected to a Biopac Systems MPS-WSW 100 hardware/software package and a Gateway 2000 120 MHz computer. Room temperature was kept between 68 and 72 degrees F. In addition, because of the live-in nature of the project, variability due to outdoor temperature was minimized. During the following week, the subjects received a variety of supervised treatments. These included 3 sessions on the Radial Appliance, dietary changes, massage, and colonic irrigations. We avoided biofeedback procedures or other interventions directed at hand-warming. At the end of the week, autonomic parameters including finger temperature were again measured according to the same protocol. Results All five subjects showed substantial increases in finger temperature at the second measurement period (mean increase 8.4 degrees F, SD = 3.3). Figure 2 shows the temperature profiles, over the 28-minute period, for the five subjects. None reported immediate relief from headaches. However, in a 6-month follow-up, the three subjects who continued with the program reported substantial relief. General Discussion The results of the two studies tend to confirm the hypothesis that the use of the Radial Appliance can warm the hands. However, the high temperature variability in both the experimental and control groups in the experimental study makes those results difficult to interpret. The results from the five subjects in the clinical study are strong and consistent, but the absence of a control group limits our ability to attribute the temperature increase entirely to the Radial Appliance. In the experimental study, several factors may have contributed to the variability. First, skin temperature is intrinsically highly variable within some individuals. While for some subjects there was little temperature fluctuation over the course of a session, for others there was wide variation. Some women who had reported previous "hot flashes" showed rather unstable temperatures during the sessions, with large changes over periods of a few minutes. The literature confirms that this is not an uncommon effect.9 Some with specific diseases, such as diabetes and Parkinson's disease, also showed unusual temperature patterns. One woman who developed eczema on one foot during the project, also developed an over-10-degree difference between her feet, the only subject to show such a difference. The criteria to exclude subjects may need to be more stringent in future experiments. In the experimental group, consistency of use of the appliance appeared to be an important factor. As noted in the Results section, many subjects failed to use the appliance as frequently as recommended by Cayce. Frequency of use was suggestively correlated with hand temperature in this group, but not in the control group, by the end of Session 16. In the control group, the occurence of substantial hand warming in some individuals can be attributed to their behavior during the home sessions. For example, one woman with a large increase reported that she had previous experience in both biofeedback and meditation, and used the 1-hour sessions to practice these techniques. Environmental temperatures, both indoor and outdoor, did not appear to be an important factor. Indoor temperature, which was intentionally kept low to induce a temperature response in the subjects, was held adequately steady. The pre-baseline and baseline periods minimized the effects of outdoor temperature. Activity level prior to the session could not be as easily controlled, however, and may have increase temperature variability in both experimental and control groups. The clinical study may have achieved more consistent results by minimizing three important sources of variability: (1) medical condition: all subjects had migraine headaches, (2) consistency of appliance use: all sessions were supervised, and (3) activity levels: all were in a residential program with planned activities, none involving strenuous exercise near the measurement periods. On the other hand, the program certainly encouraged a placebo effect, and the other therapies may have contributed to hand warming. However, the average increase in hand temperature was over 6 times higher than that in the placebo group in the previous study, and nearly twice that of the experimental group. References 1. J. P. Callan, Editorial: Holistic health or holistic hoax? Journal of the American Medical Association, 241, (1979), p.1156. 2. E. Cayce, The complete Edgar Cayce readings on CD-ROM (A.R.E. Press, Virginia Beach, VA, 1993). 3. D. McMillin & D. G. Richards, The radial appliance and wet cell battery: Two electrotherapeutic devices recommended by Edgar Cayce (Lifeline Press, Virginia Beach, VA, 1995). 4. L. E. Eeman, Cooperative healing (Frederick Muller, London, 1947). 5. L. Patten & T. Patten, Biocircuits: Amazing new tools for energy health (H. J. Kramer, Tiburon, CA, 1988). 6. J. Isaacs, & T. Patten, A double-blind study of the "biocircuit," a putative subtle-energy-based relaxation device, Subtle Energies, 2, (1991), pp.1-28. 7. H. Grady, Study of the Cayce impedance device (Fetzer Energy Medicine Research Institute, Phoenix, AZ, 1988). 8. A. J. Yates, Biofeedback and the modification of behavior (Plenum, New York, 1980). 9. P. Lomax, Neuropharmacological aspects of thermoregulation, In The nature and treatment of hypothermia. (R. S. Pozos & L. E. Wittmers, University of Minnesota Press, Minneapolis, 1983). Correspondence: Meridian Institute, 1168 First Colonial Road, Suite 12, Virginia Beach, VA 23454, (757) 496-6009. Acknowledgments: We thank the Morrison Trust, San Antonio, Texas, for their generous support.
|