Osteopathic Regulation of Physiology
This study explored the effects on physiology of "holding the vasomotor center," a historical technique of inhibitory pressure in the cervical area, intended to affect sympathetic nervous system control of circulation. Circulation, skin temperature, heart rate and breathing rate were measured in 18 participants, during holding the vasomotor in comparison with a "sham" manipulation - a gentle touching of the tops of the shoulders. There was substantial individual variability, but averaging of the responses showed increased circulation to the fingers, accompanied by increased finger temperature and a briefly reduced heart rate followed by an increased heart rate, in response to holding the vasomotor center. Touching the shoulders did not result in any circulatory or temperature changes, but did cause a briefly reduced heart rate identical to that from holding the vasomotor center. Manual therapy encompasses both structural corrections and regulation of physiology, but the regulatory aspects have received less attention than the structural aspects.[1] Nevertheless, regulation of physiology played a significant role in historical osteopathy, and has received some support from modern research. Our goal in this pilot study was to test a claim from the early osteopathic literature, as a step toward discriminating physiologically effective manipulations from those manipulations with the potential to be "sham" controls in experiments. Historical osteopathy often focused on regulation of physiology. For example, Barber [2] states: "We all agree upon the one great point, that man is a machine, and that nerve-centers have been discovered upon which a pressure of the hand will cause the heart to slow or quicken its action, from which we can regulate the action of the stomach, bowels, liver, pancreas, kidneys, and the diaphragm" (p.28). He says, "With a thorough knowledge of the various nerve-centers, and the innervation of the different tissues and organs, the osteopath is able to coordinate the nerve-force of the body. He can increase the nerve-current to almost any part of the being, and can quiet an excessive one as well" (p.23). Modern research offers some support for the effects of manipulation on physiology, reviewed in Mein et.al.[1] For example, animal work by Sato and colleagues [3-5] supports the traditional concepts of stimulation and inhibition. Working with anesthetized animals, they have traced reflexes from various types of mechanical, thermal and chemical stimulation of the skin to visceral effector organs including the heart, stomach, sweat glands, bladder, and adrenal medulla. Heart rate can be increased in anesthetized cats by stimulation of anyone of a variety of skin areas. This reflex is produced mainly by an augmentation of cardiac sympathetic efferent nerve activity. Similarly, in the anesthetized rat, Sato demonstrated inhibition of gastric contractions by stimulating the abdominal skin. Conversely, noxious stimulation of a hind paw sometimes augments gastric motility, mediated by reflex facilitation of gastric vagal efferent nerve activity. In humans, there is also some evidence for the effects of manipulation on physiology. For example, the thoracic lymphatic pump has been shown to modify immune function [6,7] and manipulation has reduced hypertension. [8,9] Purdy et al [10] demonstrated that gentle, soft tissue manipulation in the suboccipital region can result in significant changes in blood flow in the fingers, mediated by the sympathetic nervous system. In addition, Purdy et al found that even a gentle touch in the same area, without manipulation, had a measurable effect on finger blood flow. Their result is particularly interesting because it demonstrates changes in the autonomic periphery during manipulation of a dermatome unrelated to the area being measured. One important issue that has arisen from studies on the efficacy of manual therapy is that of the placebo effect and the nature of an appropriate "sham" treatment. In a recent study of the effect of chiropractic on childhood asthma, the sham treatment included soft tissue work similar to traditional osteopathic manipulation. [11] The placebo condition included, among other manipulations, "soft-tissue massage and gentle palpation" to the spine, paraspinal muscles, and shoulders; "turning the subject's head from one side to the other;" with the subject in a supine position "with the head rotated slightly to each side, . . . an impulse applied to the external occipital protuberance;" and with the subject in the prone position, "a similar impulse was applied bilaterally to the scapulae." The study yielded evidence for the efficacy of both treatments, but the authors concluded that this result demonstrated the placebo effect. We have disagreed, pointing out the importance of considering the diversity of manual techniques when studying manual therapy. [12-15] In particular, soft tissue techniques that do not involve high velocity, low amplitude (HVLA) thrusts on the spine may have significant physiological effects, as shown in the Purdy et al [10] study. We had a particular interest in techniques affecting the sympathetic/parasympathetic balance and influencing circulation, since this is an important consideration in therapy for asthma. Rather than looking at a complex, full treatment, we chose to study a simple maneuver from traditional osteopathy, in comparison with another simple maneuver not expected to have a direct effect on the sympathetic nervous system. We chose a manipulation intended to inhibit the superior cervical ganglion; a primary vasomotor center discussed in various early osteopathic manuals. [2,16-18] The vasomotor system controls the circulation of the body. Inhibition, defined as holding a steady pressure on the cervical vasomotor center, was said to dilate the blood vessels by reducing sympathetic nervous system activity, increasing circulation to such areas as the hands and feet. Barber [2] used the expression "holding the vasomotor" when referring to this technique. His description of the move was as follows: "Place the hands upon the sides of the neck, the fingers almost meeting over the spine of the upper cervicals; tip the head backward, pressing hard upon the vasomotor center four or five minutes . . ." (p.260). Figure 1, from the 1910 Text-Book of Osteopathy 19 illustrates the maneuver as we used it in the current study. The move was said to be particularly useful in treating headache and reducing fevers associated with infectious disease. A. T. Still realized the therapeutic potential of steady pressure on the cervical ganglion when he used an inhibitive technique (lying with his neck in a sling) to relieve his own headaches. [20] Later, when writing Philosophy of Osteopathy in 1899, [21] he included an entire chapter by William Smith on "The Superior Cervical Ganglion." Smith discussed the effects of inhibitory pressure upon the upper four cervical nerves: "the capillaries over the entire surface of the body flushed, this being accompanied by a fall in pulse rate and a marked diminution of the temperature [note that he does not specify which temperature - he probably means the internal body temperature]" (p.267). In another passage Smith discussed inhibition of the superior cervical ganglion, and noted that it should produce "relaxation of the vascular walls . . . the skin will become flushed and moist . . . the vagus is now allowed full sway, and we must find slowing of the heartbeat" (p.266). We had two questions. The first was whether the effects of such a maneuver
on physiology could be measured. The second was whether the maneuver of
holding the vasomotor had specific effects that were different from those
of a "sham" treatment - simply lightly touching the tops of both shoulders
simultaneously, for the same duration as the vasomotor inhibition. Note
that, like the sham treatment in the Balon et al [11] study on asthma,
these manipulations involved the soft tissue of the neck and shoulders.
Methods Eighteen volunteers (6 male, 12 female, mean age 51, SD 11.1, range 28-74) participated in the project. There were no specific selection criteria; all participants were questioned concerning any conditions that might affect circulation. Although several reported poor circulation to the extremities, these participants were included since a possible change in circulation was relevant to the hypothesis. All participants provided informed consent prior to their participation; the consent form included a statement that the experiment had no therapeutic purpose, but was solely to collect physiological data. Each person took part in one or two sessions, as described below. Physiological measurement was performed using a Biopak Systems MP100WSW data acquisition system. Measures included heart rate (calculated from electrocardiograph beat-to-beat interval), depth of breathing (from temperature measurement of inhalation and exhalation through the nose), circulation to the finger (right thumb) and toe (right big toe) from a photoplethysmograph, and temperature of left thumb. Room temperature was maintained at between 68 and 73 degrees F (20.0 and 22.8 degrees C). This was intended to provide a slight thermal stress, cooling the extremities. The subjects were instructed to lie on a table for 40 minutes, while
we measured the physiological variables. They were told to simply relax.
After a 10-minute baseline, a therapist would either hold the vasomotor
center, or lightly touch the tops of the shoulders, for 5 minutes. The
order was randomly chosen to avoid effects simply due to how long the person
had been lying on the table. Then, after another 10-minute period of relaxation,
the other manipulation would be given for 5 minutes, and the session would
end with a final 10-minute period of relaxation.
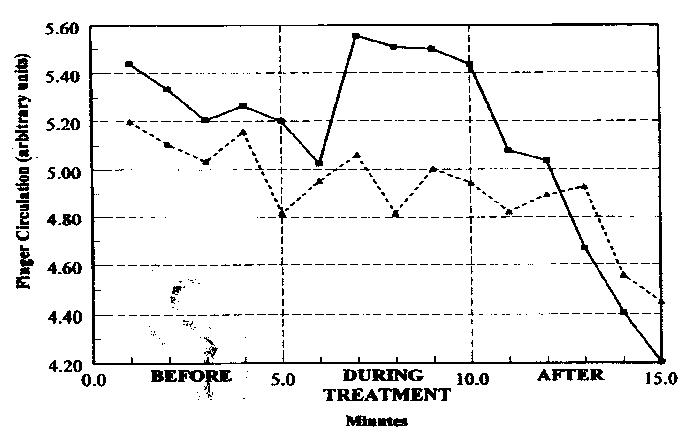
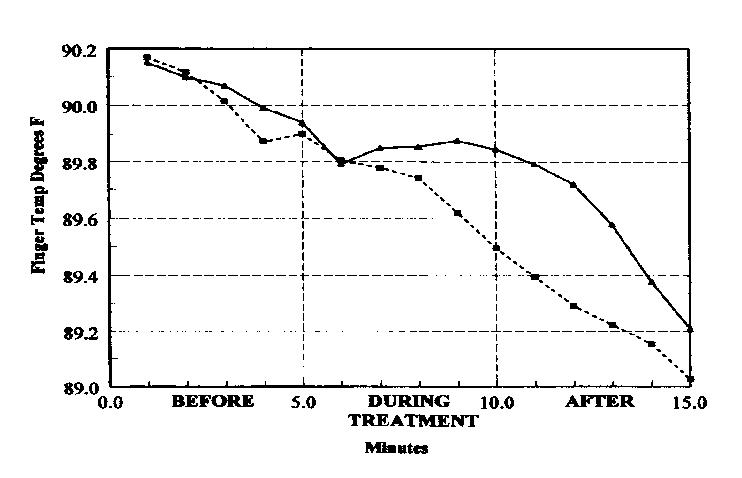
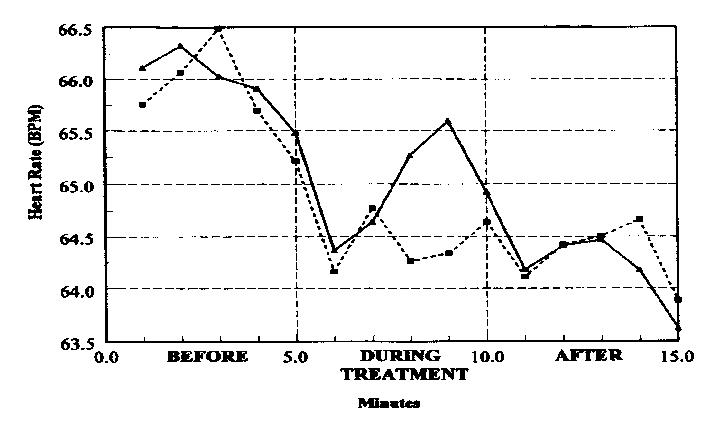
Results The most striking result initially was the presence of a great deal of individual variability. For example, the baseline finger temperature ranged from 74 degrees F to 96.5 degrees F. But by averaging over many sessions (23 total sessions in this report), we were able to clearly see the typical effects of these maneuvers on physiology. Over time, with no treatment at all, circulation and skin temperature tend to drop in a cool room, and heart rate decreases as the body relaxes. We were looking for departures from this general trend. Figure 2 shows the average effect on finger circulation. The standard deviation of the blood volume pulse from the photoplethysmograph was used as a measure of circulation. The graph shows 5 minutes before the treatment, the 5-minute treatment, and 5 minutes after the treatment. Holding the vasomotor is the solid line; the shoulder touch is the dotted line. The graph shows that, on the average, about a minute into the treatment, circulation goes up with the active treatment, while it stays the same with the sham treatment. Figure 3 shows the average effect on finger temperature. The means have been adjusted to show identical temperature at the beginning of the measurement period. Note that the effect on temperature is smoother and longer lasting than the one on circulation. It takes a while for the flow of blood to the surface to actually warm the skin, and then the skin holds heat longer after the blood flow has decreased. Figure 4 shows the effect on heart rate. This
was especially interesting to us, since in the first minute of both maneuvers,
heart rate decreases. A decrease of heart rate is consistent with the historical
osteopathic literature. [21] However, here it seems to be a general response
to being touched. Then heart rate increases for the "holding the vasomotor"
maneuver, while for the shoulder touch there is no change.
Discussion The early osteopaths made strong claims about the effects of manipulation on physiology. This pilot study provides evidence that, with an average of many subjects, the circulatory effects of holding the vasomotor center can be demonstrated. However, the variability both within and between subjects was so great that caution must be exercised in accepting any generalization about effects. It is also clear that treatments involving the neck and shoulder, including ones intended as sham treatments, have the potential for physiological effects and should not be thought of as placebo controls. Variability - both baseline variability unrelated to the manipulation, and variability in response to the manipulation - is the greatest challenge in this research, making statistical analysis difficult. Driscoll and DiCicco, [22] who are also exploring the effects of manipulation on physiology (heart rate variability), faced a similar problem of variability that swamped the desired effect. They were able to reduce the variability by driving heart rate with timed breathing, but noted that this may override any effects from manipulation. We are exploring ways to reduce variability by selecting subjects based on preliminary measurements of physiology. Another significant issue raised by the results concerns the time frame of the measurements. The baseline must be sufficiently long to establish a trend or to allow the variability to stabilize. The treatment period must be sufficiently long for an effect to occur, but not so long that the response habituates or reverses. For example, in a preliminary experiment we found a reversal effect, where inhibition would appear about halfway into a 10-minute period of stimulation. The measurement period must be sufficient to allow for any lag between the treatment and the response, and for any persistence of the effect after the end of the treatment. For example, a study by Harris and Wagnon [23] looked at finger temperature 10 seconds after an HVLA chiropractic adjustment, finding evidence of physiological effects. Our data suggest that even with a rapid increase in peripheral circulation, there is a lag of 30 seconds or more for temperature to rise, making their results difficult to interpret. Finally, persistence of effects can complicate studies in which a series of manipulations are given. The heart rate result shows how hard it may be to define a "sham" treatment
for scientific study. Our sham maneuver was a light touch of the tops of
both shoulders, which is not a location of significance in the osteopathic
literature. The shoulder touch response is likely to be a nonspecific reaction
to being touched, but there remains the possibility of specific effects
on the autonomic nervous system from points distant from the spine. As
noted previously, Purdy et al [10] found that a light touch on the occipital
area had an effect on digital blood flow. Several participants in the current
project pointed out that the points of shoulder contact might be relevant
in acupressure. Alternatively, some of the Chapman's points used in osteopathic
manipulative therapy bear little obvious relation to the target organ.
For example, the anterior points for the eye problems of retinitis and
conjunctivitis are located on the front of the humerus,24 (p.18). Even
light stroking of the skin has claims of major effects on lymphatic physiology.
[25] We concur with Purdy et al [10] that manipulation of the cervical
area can have useful physiological effects, and could be applicable to
the treatment of entities such as migraine or other hyperautonomic states.
In addition, it is clear that even simple touching is not an inert placebo,
and that the effects of touching itself bear further investigation.
References 1. Mein EA, Richards DG, McMillin DL, McPartland JM, Nelson CD. Physiologic regulation through manual therapy. Physiological Medicine and Rehabilitation: State of the Art Reviews. 2000:14:1:27-42. 2. Barber ED. Osteopathy Complete. Kansas City, MO. Press of Hudson-Kimberly Publishing Co. 1898. 3. Sato A. Somatovisceral reflexes. J Manipulative Physiol Ther 1995:18:597-602. 4. Sato A. Reflex modulation of visceral functions by somatic afferent activity. In: Patterson, MM, Howell, JN, editors. The Central Connection: Somatovisceral/Viscerosomatic Interaction. 1989 International Symposium. Athens, Ohio: American Academy of Osteopathy. 1992:53-76. 5. Sato A, Sato Y, Suzuki A, Uchida S. Neural mechanisms of the reflex inhibition and excitation of gastric motility elicited by acupuncture-like stimulation in anesthetized rats. Neurosci Res. 1993:18:53-62. 6. Measel JW, Jr. The effect of the lymphatic pump on the immune response. I. Preliminary studies on the antibody response to pneumococcal polysaccharide assayed by bacterial agglutination and passive hemagglutination. JAOA. 1982:82:1:28-31. 7. Jackson KM, Steele TF, Dugan EP, Kukulka G, Blue W, Roberts A. Effect of lymphatic and splenic pump techniques on the antibody response to hepatitis B vaccine: A pilot study. JAOA. 1998:98:155-160. 8. Mannino JR. The application of neurologic reflexes to the treatment of hypertension. JAOA. 1979:79:225-231. 9. Morgan JP, Dickey JL, Hunt HH, Hudgins PM. A controlled trial of spinal manipulation in the management of hypertension. JAOA. 1985:85:308-312. 10.Purdy WR, Frank JJ, Oliver B. Suboccipital dermatomyotomic stimulation and digital blood flow. JAOA. 1996:96:5:285-9. 11.Halon J, Aker PD, Crowther ER, Danielson C, Cox PG, O'Shaughnessy D, Walker C, Goldsmith CH, Duku E, Sears MR. A comparison of active and simulated chiropractic manipulation as adjunctive treatment for childhood asthma. N Engl J Med. 1998:339:1013-1020. 12.Richards DG, Mein EA, Nelson CD. Chiropractic manipulation for childhood asthma [Letter]. N Engl J Med. 1999: 340:391-392. 13.Nelson CD, McMillin DL, Richards DG, Mein EA, Redwood D. Manual healing diversity and other challenges to chiropractic integration. J Manipulative Physiol Ther. 2000:23:3:202-07. 14.Mein EA, Greenman PE, McMillin, DL, Richards DG, Nelson, CD. Manual medicine diversity: research pitfalls and the emerging medical paradigm. JAOA, in press, 2001. 15.McMillin DL, Richards DG, Mein EA, Nelson CD. [Letter]. The AAO Journa1. 2000:10:11-12. 16.Hazzard C. Principles of Osteopathy (Third Edition). Kirksville, MO, Charles Hazzard, 1899. 17. Feidler FJ. The Household Osteopath. New York. Broadway Publishing Company. 1906. 18. Davis AP. Neuropathy. The New Science of Drugless Healing Amply Illustrated and Explained. Cincinnati, OH. F. L. Rowe. 1909. 19. Text-Book of Osteopathy. Chicago, IL, American College of Mechano-Therapy, 1910. 20. Still AT: Autobiography of Andrew Taylor Still. Kirksville, MO. A. T. Still. 1897. 21.Smith W. Chapter 20 - The Superior Cervical Ganglion. In Still AT, ed. Philosophy of Osteopathy. Kirksville, MO, A. T. Still, 1899. 22. Driscoll D, DiCicco G. The effects of metronome breathing on the variability of autonomic activity measurements. J Manipulative Physiol Ther. 2000:23:610-614. 23.Harris W, Wagnon RJ. The effects of chiropractic adjustments on distal skin temperature. J Manipulative Physiol Ther. 1987:10:57-60. 24.Kuchera ML, Kuchera W A. Osteopathic Considerations in Systemic Dysfunction. Kirksville, MO. KCOM Press. 1991. 25.Kurz I: Textbook of Dr. Vodder's Manual Lymph Drainage. Volume 2:
Therapy. Brussels. Hang International. 1986.
Note: The complete texts of the historical sources on osteopathy are
all available on the Meridian Institute web site, www.meridianinstitute.com,
in the Early American Manual Therapy section.
|